Statutory Reporting fields can be found in various spots across the patient record. These drop downs contain only values that are valid for the statutory reporting bodies that you submit to. You will not be able to modify the contents of these drop downs as they are set by reporting bodies.
Example Statutory Report Fields in the Patient Record are:
- Marital Status
- Country of Birth
- Indigenous Status
- Preferred Language
Statutory Reporting fields can also be found in the admission screens:
- Admission Date
- Admission Time
- Urgency of Admission
- Source of Referral
- Inter-hospital Contracted Patient
- Re-admission Within 28 Days
- Same-day Status
- Hospital Insurance Status
- Contracted Patient Status
- and the list goes on...
If the chosen report to run has already been generated and submitted, or there are errors in the generation, a message with the specific details will be provided. All admission details can also be shown by clicking on Show All.
Regeneration of a report (as long as it has not been submitted and accepted), will invalidate the previously run report.
Linking an Admission to an Invoice
For HCP reporting, every admission which has charges raised (invoice) needs to be report them. This is achieved by linking the admission to the invoice.
Behind the scenes, when the HCP report is generated, charges are passed through in the extract. Typically, the invoicing relates to the IHC portion of the claim - Theatre and Accommodation.
This means that before you can successfully generate an reporting extract, all admissions within that period must have an invoice linked to them.
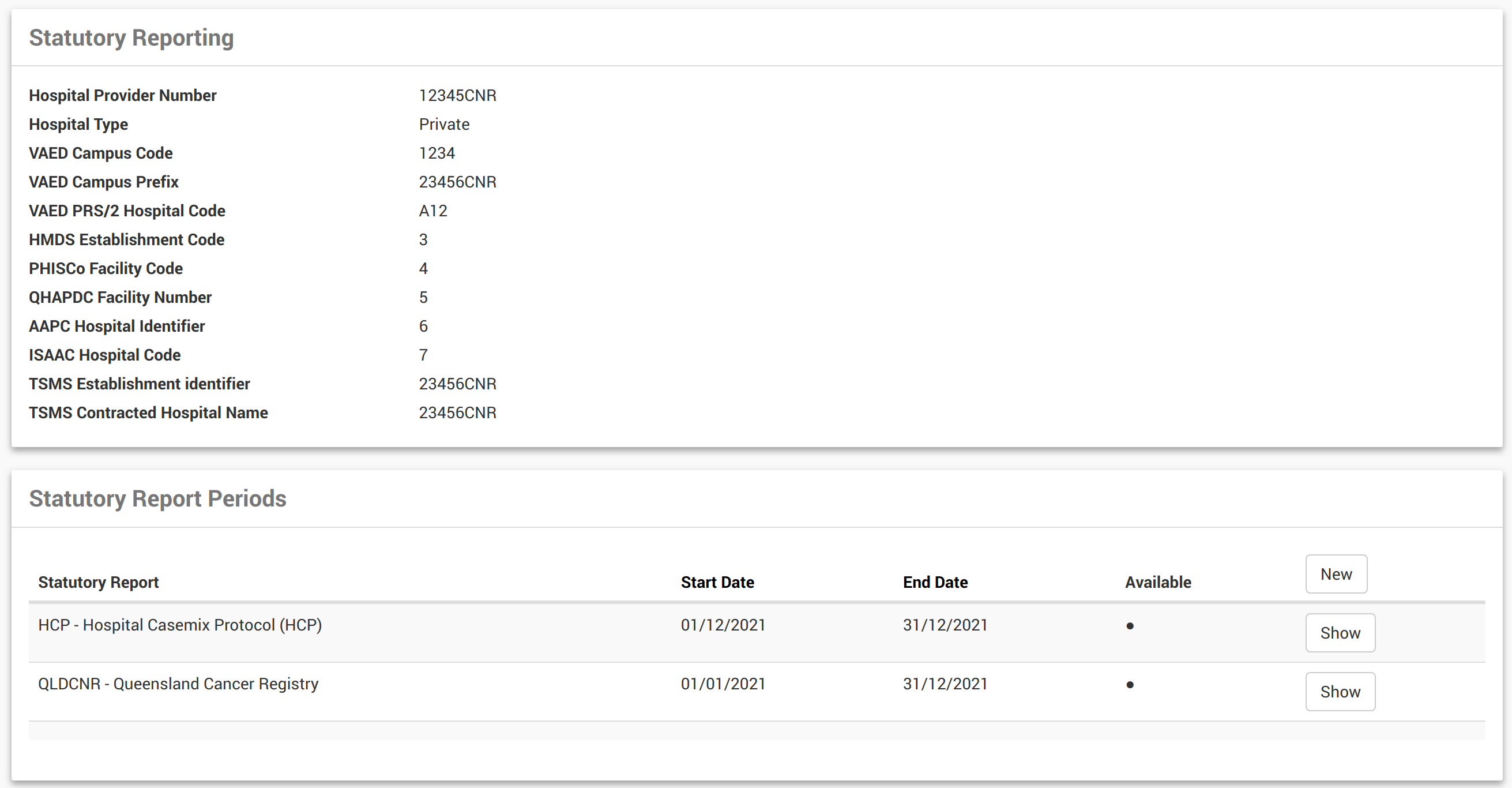
- From the Locations menu, find and Show location.
- Click on Statutory Reports from the menu.
- Details of last run reports will be displayed.
This page displays eligible reports including the date period of the most recently generated report (if any have been generated). New reports can be generated from here or historical reports, if there are any, can be viewed.
If the chosen report to run has already been generated and submitted, or there are errors in the generation, a message with the specific details will be provided. All admission details can also be shown by clicking Show All.
Statutory Report Record Interface
| Field Name | Description |
| Report | Report name and version. |
| Date | Date when the report was created. |
| Contents | Displays the name of the report and the report version. |
| Generated At | Displays when the report was last generated. |
| Action Column | Actionable button enabling user to reject the record or informational text conveying that the record was rejected. |

Running Reports with Non-discharged Day Surgery Patients
A warning message will appear—and the report will not run—if there are still day surgery patients not yet discharged.

CareRight prevents you from running a statutory report within the current month. Due to a nuance with time zones, you need to wait until 12pm EST on the first of the month before running the report for the previous month.
So, if you want to run the report for admissions for November 2017, the earliest you can run this report is 12pm EST on December 1st 2017.
Statutory reporting is the mandatory submission of financial and non-financial information to a government agency. The health industry in Australia has its own set of laws and regulations that mandate the format and the data of statutory reporting.
CareRight supports each states legislation for submitting statutory reports:
- AAPC - ACT Admitted Patient Care Data Collection
- HCP - Hospital Casemix Protocol
- HMDS - Hospital Morbidity Data System
- ISAAC - Integrated South Australian Activity Collection
- PHISCo - Private Hospital Inpatient Statistic Collection
- QHAPDC - Queensland Hospital Admitted Patient Data Collection
- QLDCNR - Queensland Cancer Registry
- TAS - Tasmania Statewide Morbidity System
- VAED - Victorian Admitted Episodes Dataset
Statutory reporting is mandatory for all practices or specialists who deliver any type of surgery.
Reporting Criteria
The reports will generate days of admission based on each state requirements (i.e. taking into consideration if a patient has a leave day). Reports are also based on discharge date, not admission.
Initial Setup
Prior to running statutory reports, your System Administrator must complete a few steps:
- Create Locations which need to provide reports.
- Ensure each Location has a Hospital Provider Code and legislation code(s) defined.
- For System Administrators, to add a reporting period, System Administration > View location > Select New
- For System Administrators, to add a reporting period, System Administration > View location > Select New

Permissions
Statutory Reporting and access permissions will be assigned by your System Administrator. Please refer any access queries to your System Administrator.
State Base Cancer Registry Reporting (Notifications)
CareRight has been configured to run Cancer Registry reports utilising the existing Statutory functionality - See Running Reports - Cancer Registry
Holding Admissions from Extract
These may be ‘admissions’ that we have a contract with the Health Fund and billed as Outpatient Medical Services (OMS). These are not usually admitted and therefore aren’t required to be reported to State Health. We have to admit and code these ‘admissions’ so that the Health Fund will pay. The Health Funds have advised that they do not require us to send these through HCP.
This is now supported by making an Outpatient admission.
- Set the same day status to Non-admitted. These are excluded from stat reporting.
- To claim you may need to set the optional field Service Category to 6 on the IHC claim form.
Gender Definitions
CareRight uses gender options that are aligned with standards established by the Australian institute of Health and Welfare. These are:
- Male
- Female
- Other
Consolidated Change Reporting for VAED Reports (v6.67.3 Enhancement)
The Victorian Department of Health and Human Services require that VAED monthly reports include changes to previous admissions, when applicable. In order to support this directive, CareRight now offers consolidated change reporting for VAED statutory reports.
Regenerating Reports
When regenerating reports, only the last month's report for that financial year will be available for regeneration. This means that the report for June for any year can always be regenerated and submitted to VAED, provided that it has met eligibility for its initial creation.
Note in the example below, the Regenerate button is hidden when there is a more recent report within the financial year, though June is still available for regeneration.

Include Entire Admission History
When the Include entire admission history for YTD checkbox is selected, then all admissions for that financial year up to the end of the current reporting month will be included in the VAED report, even if they have not been changed. By default, this option is unchecked.

Run individual fund HCP extracts (v6.69.3 Enhancement)
There are instances where hospitals may not be able to bill some admissions while negotiating health fund contracts, however. they still need to submit statutory reporting for those admissionons. Pre 6.69.3 is not capable of generating statutory reports if any of the fund's admission has no invoice.
6.69.3 Enables this feature where the following set of rules will be applied.
The following fields will be filled as $0
- HCP/PHDB > accommodation_charge
- HCP/PHDB > theatre_charge
- HCP/PHDB > labour_ward_charge
- HCP/PHDB > intensive_care_unit_charge
- HCP/PHDB > prosthesis_charge
- HCP/PHDB > pharmacy_charge
- HCP/PHDB > other_charges
- HCP/PHDB > bundled_charges
- HCP/PHDB > hospital_in_the_home_care_charges
- HCP/PHDB > special_care_nursery_charges
- HCP/PHDB > coronary_care_unit_charges
The funding source will be determined as follows:
If the admission has a pre-admission and the preadmission identifies the guarantor then that guarantor is used to determining the payer identifier.
If the admission has no pre-admission and the patient has health fund details recorded then assume the admission will be billed to that health fund and use that the payer identifier.
If the admission has no pre-admission and the patient has no health fund details recorded then assume the patient is paying and sen the payer identifier as self-insured.
The following report fields will use the determined funding source:
- HCP/PHDB > insurer_payer_identifier
- AAPC > funding_source
- HMDS > funding_source
- ISAAC > funding_source
- QHAPDC > funding_source
Invoicing Change
When creating an invoice that is linked to an admission ensure the admission is flagged for resubmission.
Note: Having no invoice no longer raises an error when generating stat reports and detail the rules described.
For clients collection data for VAED data submissions it is important to understand how the VAED locality is collected and managed for an Admission. If a VAED location cannot be identified for a patient the VAED report will not generate until the user has manually set a VAED locality.
CareRight contains a list of all defined VAED locality as published by the Victorian Government.
Vaed requires all patients:
- admitted in the month
- are currently admitted in the month
- any changes to other admissions previously submitted to VAED in the current financial year.
It is important for Australian addresses that the patient's home address is set to the correct address. For addresses within Australia it is recommended that you first search using the patients suburb name as this will automatically search and match the VAED locality list and ensure that the address will be compliant.
On / After Discharge
When you EDIT an admission after discharge CareRight will use the residential (home) address taken at discharge for the Patient to determine the best fit VAED locality to use using prefilll rules When you save the Admission this data is recorded for the admission.
Before Discharge
The VAED Locality will attempt to set a value on Admission and users can change this by editing the admission, but note: this value may change if the user updates the patients home address postcode and or suburb before they are discharged. Each time a VAED report is generated and the admission is included in the VAED report being generated the home address:
- postcode
- suburb
are checked for changes . If they have changed then it will change the VAED locality using the prefill rules.
Prefill Rules used when per-selecting VAED locality
The following rules are used to prefill the VAED locality information:
- If the Patient has no home address then the VAED Locality is left blank. The drop down options for the VAED Locality will contain "No Fixed Abode" and "Unknown" to allow the user to record the reason why they have not been able to collect the locality information of the Patient.
- if the Patient has a home address with country Australia, but the postcode / suburb does not match the contents of the VAED Locality list then the VAED Locality will be left blank and there will be no options available to select from.
- if the Patient has a home address with a country other than Australia then the VAED Locality will attempt to match the correct country based on description with the VAED Locality list.
Fixing Errors
Fixing incorrect VAED Locality information:
If the VAED Locality is recorded incorrectly the best course of action to resolve is to:
- Ensure the patient's home address details are updated to the correct address
- Edit the Admission and remove any existing VAED Locality information and SAVE the admission
- Edit the Admission a second time and ensure the VAED Locality has not updated correctly and SAVE the admission.
Mandatory Statutory Reporting values with error - that are configured to be hidden will now be visible when you run the report!
In some cases, Admission Categories value that are configured to be hidden but are mandatory values for Statutory Reporting will have validation errors. For these hidden values, users are now shown and prompted which values and records require action.
For example: Care Type is a hidden field.

You can click on the admission link and edit and under Admission Category Configuration, tick Display Hidden Fields

Edit the field required.

CareRight aims to provide comprehensive and compliant statutory reporting; but does not cover all aspects of all requirements.
Admissions
Last reviewed: June 2025
Special Care Nursery Charges
Currently, these are a manual entry rather than calculated from admission line items.
Coronary Unit Care Charges
Currently, these are a manual entry rather than calculated from admission line items.
QHAPDC
Last reviewed: August 2025
SNAP - Maintenance Care
CareRight does not support the modelling and generation of Maintenance care SNAP Records; as the system only models a single episode.
SNAP - Rehabilitation
Rehabilitation is not modelled in the system - specifically Primary Impairment Type
APC / ISAAC
Last reviewed: June 2025
Prison/Remand/Youth Training Centre
CareRight does not capture fine grained definitions beyond Custodial
Infant Weight
The system allows data capture for this, but it is not currently reported.
HMDS
Last reviewed: June 2025
Update flag not supported
Mother's Identifier not supported
Continuous ventilatory support hours not supported
Contracted Care Flag - Private hospitals not required to submit.
PHISCO
Last reviewed: June 2025
ICU hours are not currently mapped.
Unqualified Newborn Bed Days are not currently mapped.
Episode deletion not supported.
Daily Usage
This article explains the workflow associated with collecting the data for PCOC statutory reporting.
Please note: PCOC Data capture needs some system Administration configurations. Please review Here . |
1. Add Diagnosis information;
Diagnosis can be entered in the patient Field 'Diagnosis' under the Demographics session.

2. SLK
Automatically generated from Patient information. See SLK Usage Guide.

3. Creating a PCOC Episode on Admission
- Create your admission
- Select the field Care Type: Palliative (This can be defaulted in Admission Category level)
- Tick PCOC assessments conducted (in Admission Category level)
- View the admission
- Provided you have PCOC Editor permissions, you will be presented with the ability to Create a new PCOC Episode from this Admission

4. Click on PCOC Episode, this will create a PCOC Episode.

4. Creating a PCOC Episode outside of an Admission
If required, an episode can be started outside of the context of an admission.
View Patient > PCOC Episodes > New.

5. Capturing Observations via the PCOC Assessment
Once the patient is admitted for Palliative Care, the daily observations and phase changes can be monitored and recorded through an assessment, which is capable of managing the phases in associated PCOC Episode.
Please contact Clintel to configure this assessmenta nd associated trigger.
The Record Phase Change button will open two tabs (this requires popup blocking to be turned off on browser)
- One for ending the existing Episode Phase (Add Phase End Date etc..)
- One for creating new episode Phase.

6. Recording PCOC Episode Phase changes manually (Without using Assessments)
View the PCOC Episode
Choose one of "Move to (phase)" or alternatively click "Add" in the PCOC Phases section.

You are presented with the ability to capture phase information.

Completing a PCOC Phase
View Patient > PCOC Episodes > Show > Identify the correct phase > Actions > Edit

Generally this information will be recorded by staff making the decision to record a phase change, via the assessment processes.
When an end date is specified, a number of other fields are considered mandatory.
Completing a PCOC Episode
View Patient > PCOC Episodes > Identify the correct episode > Actions > Edit
Here you are able to key in the final details of the Episode.

Statuatory Reporting
PCOC
Available under Locations > Statutory Reporting.

QHAPDC
Automatically generated from the PCOC Phases.
